
[cmamad id=”18200″ align=”center” tabid=”display-desktop” mobid=”display-desktop” stg=””]
And you can get a year’s supply for $15
—-Important Message—-
My blood pressure: My doctor freaked out and the nurse was calling 9-1-1…
Well, I THOUGHT the nurse was calling 9-1-1.
But I was totally wrong.
The doctor asked me, “What have you been doing differently?” I told him.
He said, “Well, keep doing it. But I’m worried…”
“Now your blood pressure is TOO LOW…”
“I’ve never seen blood pressure drop like this. Let’s stop the blood pressure medication altogether. Stop taking what I gave you. Now.”
The next day, I felt better than I had in a long, long time.
And my blood pressure was normal for the first time in years.
In fact, from that day forward, I have never had to take anything for my blood pressure.

———–
This energy drink ingredient is giving men their erections back
We have had a comprehensive understanding of gallstone formation for decades.
As with nearly all medical conditions – such as cancer or arthritis – knowing the underlying cause readily suggests the cure.
And as with many conditions, scientists discovered the cause of gallstones during the decades spanning the ’60s and ’80s…
And then ignored it for profit reasons.
Likewise, Big Pharma and the medical industrial complex have deliberately obscured the causes of Alzheimer’s disease, cardiovascular disease, and diabetes type 1 on an ongoing basis.
“The effort expended by clinicians to provide treatment for patients with biliary tract calculi has thus far outdistanced that directed toward research into the basic mechanisms of gallstone formation.”
What we know about gallstone formation and dissolution lies on a solid scientific foundation, one perfectly concordant with all epidemiological data.
We can predict gallstones by diet and blood chemistry alone. And we can reliably dissolve them within months – easily, safely, and affordably.
The processes of gallstone formation and dissolution are so simple that everybody should know the cause, or at least the cure.
Yet, with a $6.5 billion industry in the balance, it’s no wonder it remains obscure to most of us.
Only the population of mainland Japan seems to know, as a whole.
And that’s because they are basically the only population who routinely prevent the cause of gallstones via supplements.
[cmamad id=”18201″ align=”center” tabid=”display-desktop” mobid=”display-desktop” stg=””]
“Gallstone disease is common: >700,000 cholecystectomies and costs of 〜$6.5 billion annually in the U.S. …Ten to fifteen percent of white adults in developed countries harbor gallstones.”
Gallstones are mostly cholesterol stones.
And their formation is predominantly caused by the specific ratio of bile salts, phospholipids, and cholesterol within the bile.
Bile salts and phospholipids are polar lipids. As such, they will both form micelles when placed in water.
This occurs because the polar “head” group is attracted to the equally polar H2O solvent.
And at the same time, it repels the lipid “tails.”
The lipid “tails” are sometimes said to “attract each other” out of convenience.
But, really, it’s more like water associating with the “heads” and with itself – while ignoring and excluding the “tails.”
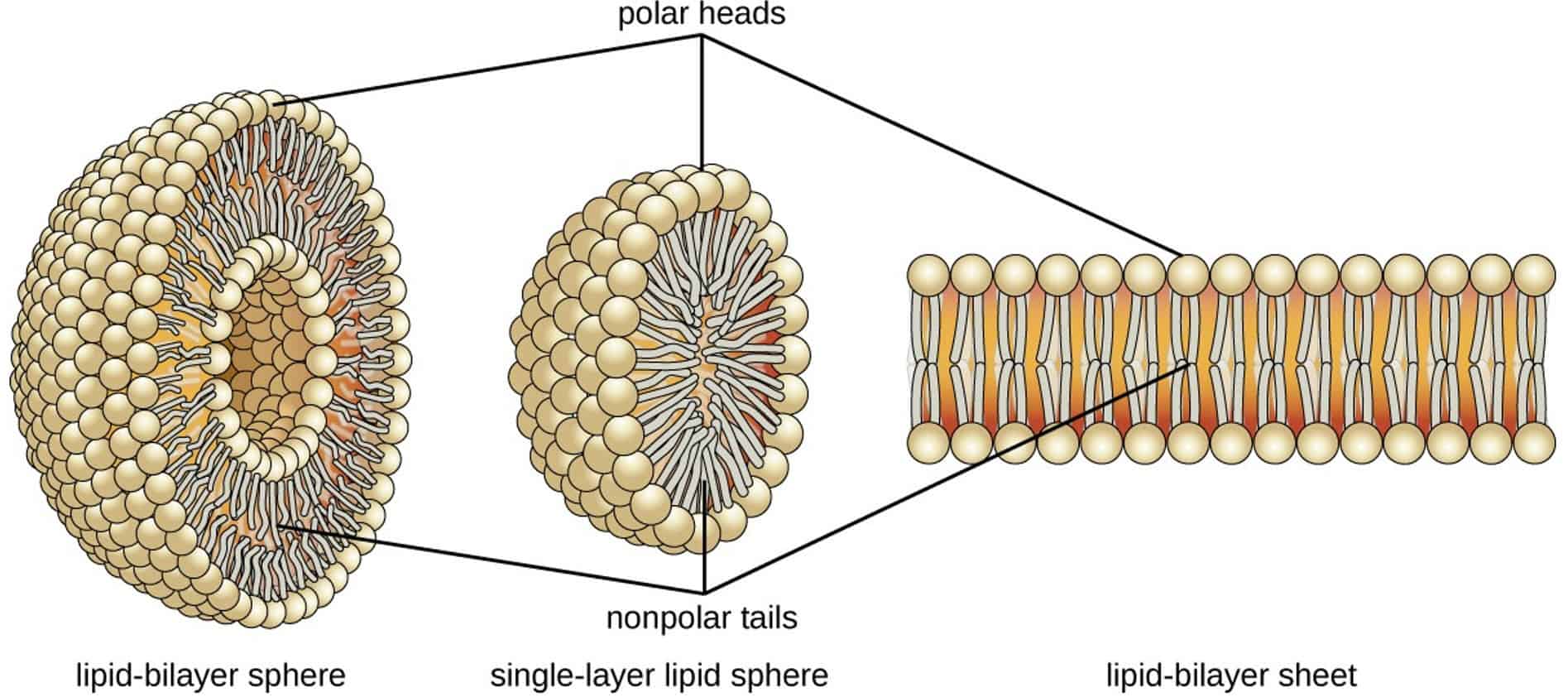
Micelles can trap cholesterol in its center.
Cholesterol is soluble in lipids but it is not water-soluble.
As such, cholesterol needs a micellar or liposomal carrier to become dispersed into solution.
When bile salts and phospholipids don’t outnumber cholesterol 11∶1 when added together, cholesterol will become supersaturated and precipitate out as gallstones.
This is similar to crystal growth in a cave, forming layer upon layer throughout time as long as pathological bile conditions favor this.
You can pretty much think of a gallstone as a “cholesterol crystal” – one initially “seeded” by a certain bile protein always found at its center.
The evidence demonstrating this is so strong that it is worth considering:
Although work on this mechanism started in 1962, it was five years later when Admirand and Small integrated all data into one intuitive model.
They found little correlation between stone formation and cholesterol-to-phospholipid ratio, and also cholesterol-to-bile-salt ratio. Yet, after phospholipids and bile salts were added together, they’d found a perfect match against cholesterol solubility.
Gallstone formation depends on the ratio of cholesterol against the combined concentration of phospholipids and bile salts.
Using purified phospholipid, cholesterol, and bile salts, they were able to determine the concentrations in which they are all soluble in water together.
The researchers dubbed this region the “micellar zone” – it represents every acceptable concentration in which all cholesterol present is found within the micellar core.
When plotted using a three-coordinate system, a line of demarcation can be drawn between the cholesterol-soluble and cholesterol-insoluble bile profiles:
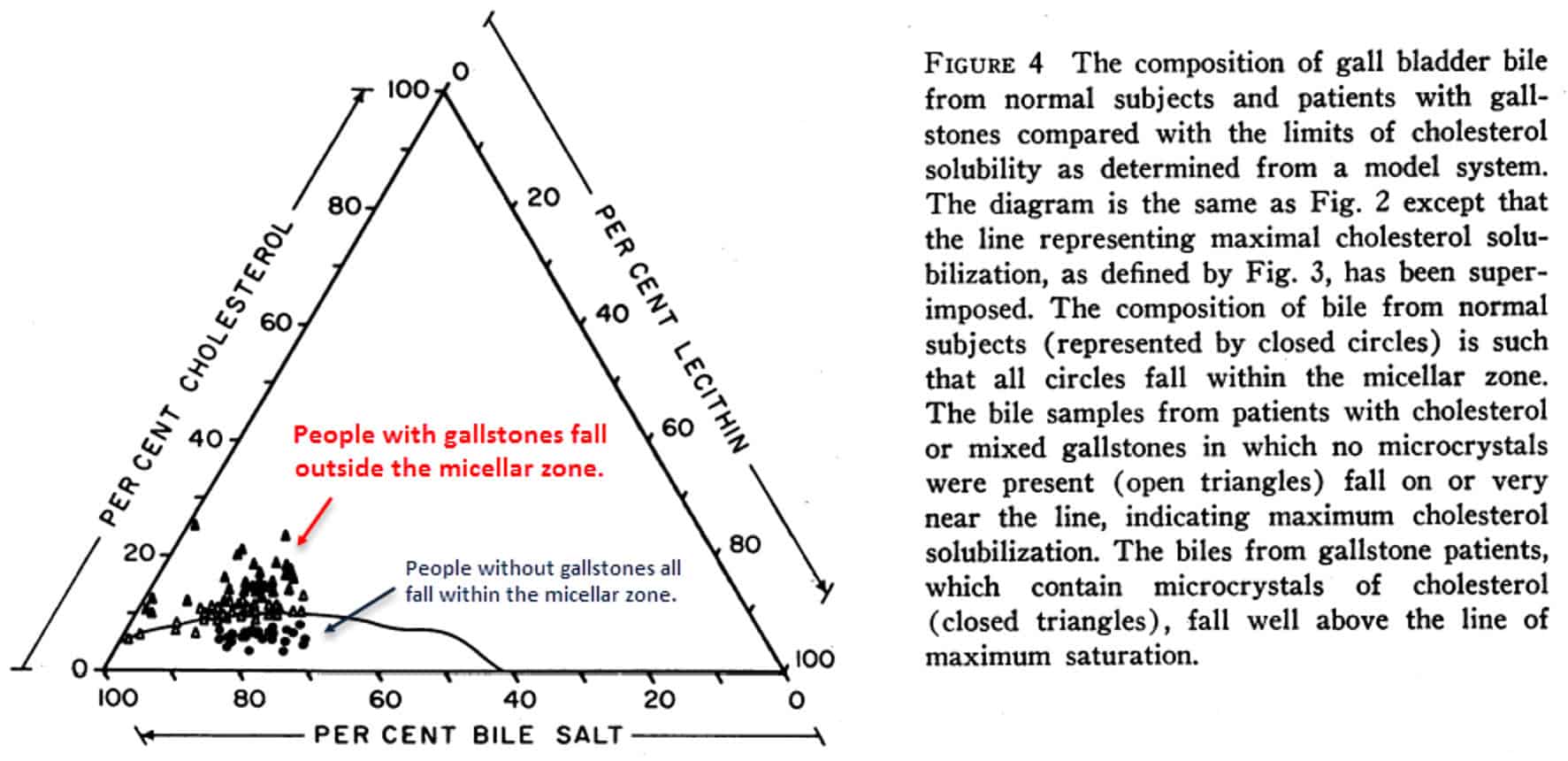
And after plotting the bile profile of subjects with gallstones, it is always found that the dots lie outside the micellar zone.
This is the “supersaturated region,” or all conditions where cholesterol becomes insoluble and precipitates.
Conversely, people without gallstones invariably lie safely within the region of micellar cholesterol solubility.
When all cholesterol is safely within micelles, there is none left to precipitate out as stones.
This has been confirmed by other researchers – in humans (Carey, 1978), non-human primates (McSherry, 1971), and prairie dogs (Lee, 1981).
The observation that gallstone formation is determined by solubility ratios is consistent – and backed by sound physicochemical theory.
However, as convincing as that all is, a wildcard in gallstone formation was suggested as early as 1976.
Extremely detailed studies were conducted ten years later – studying everything from Na+ (blood sodium) concentration to temperature.
Those studies noted significant variability within the metastable region:
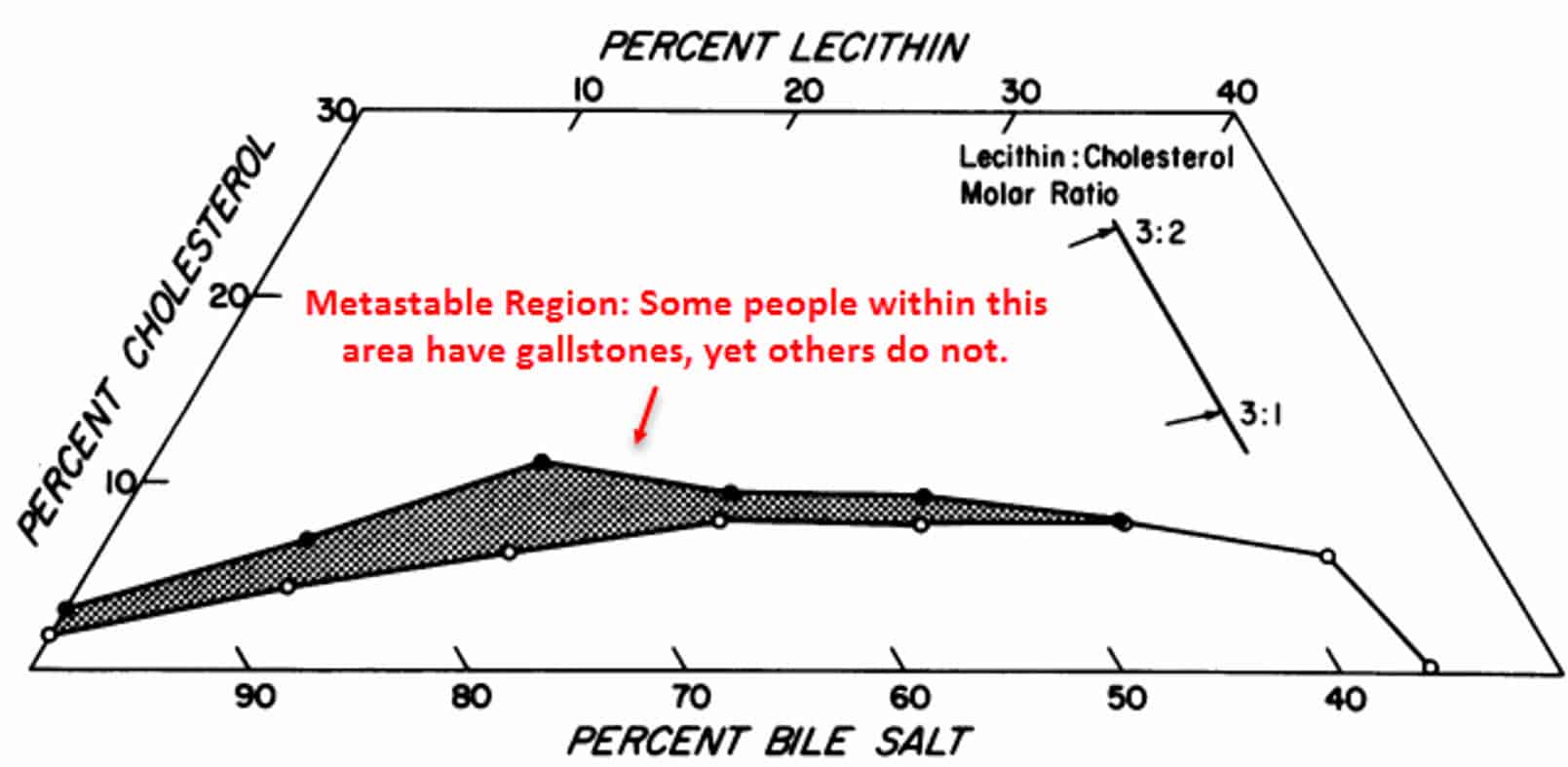
Within the boundary region of bile profiles, they found an area where precipitation would happen sometimes but not always.
In addition, people with bile profiles falling within this “metastable” region sometimes had gallstones and sometimes they did not.
So this region required further investigation.
“This suggests that the presence of certain other quantitatively minor components in human bile or the absence of nucleating agents maintain cholesterol in metastable supersaturated solution in most individuals.”
It only took five years more for researchers to discover exactly what was responsible for determining stone formation within the boundary region.
The wildcard in gallstone formation turned out to be mucin, a glycoprotein:
In the study above, the researchers induced gallbladder stones in prairie dogs by lacing their food with cholesterol.
After that, they removed and tested some bile daily.
The researchers noted a wave of mucin secretion on the fifth day – coinciding with microscopic gallbladder stones.
These kept increasing in size until the termination of the study.
“These, in turn, gave rise to cholesterol monohydrate crystals within 18 hours. Control supersaturated hepatic bile could not be nucleated by the addition of other proteins…and was stable for days upon standing.”
They also found that reconstituted bile – supersaturated with cholesterol yet stable – would precipitate upon adding mucin…and would not with any other protein.
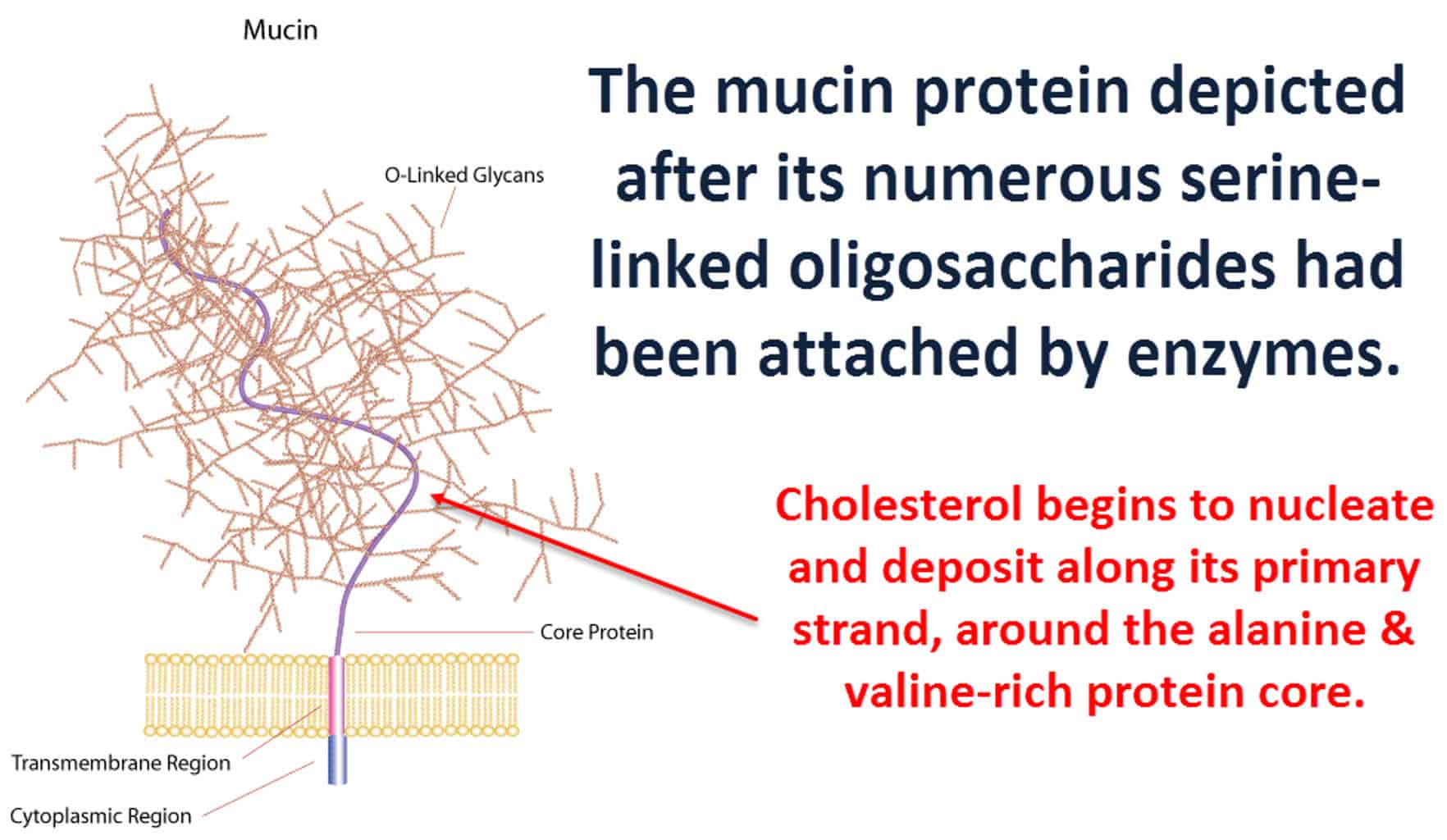
Mucin is a glycoprotein.
It has a protein core surrounded by saccharide chains arranged like a pipe brush.
The central protein strand is rich in alanine and valine (both very lipophilic).
And this area readily affiliates with cholesterol.
Mucin is at the center of nearly every gallstone.
It is the component that gives gallstones more stiffness that pure cholesterol stones.
Mucin tends to adhere to the gallbladder wall – remaining in place even after emptying the bile.
Of course, if microscopic stones are released into the intestines daily, they don’t matter much.
Yet the mere presence of mucin holds the small stones in place until they can grow into centimeter-sized larger ones.
“Cholesterol stones often contain alternating layers of cholesterol crystals and mucin glycoprotein.”
Using radio-labeled N-acetylglucosamine, Lee and Carey proved beyond any doubt that mucin synthesis coincides with the moment of cholesterol supersaturation.
However, they couldn’t explain in detail (back in 1981) why this should happen…
Other than suggesting nebulous “membrane effects” of some kind.
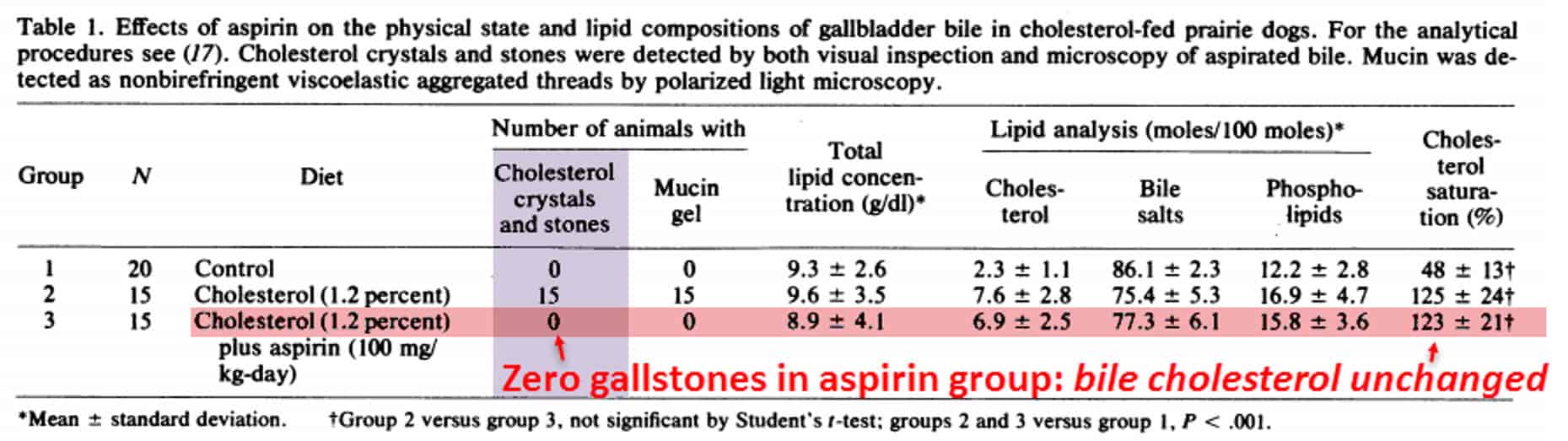
Yet, the same author showed earlier that same year that good old aspirin could completely prevent stone formation in cholesterol-fed prairie dogs:
Enough data had accumulated since then to understand the process.
Scientists now know that too much membrane cholesterol can displace arachidonic acid from the cell membrane (Chong, 1999) – the first prerequisite for prostaglandin formation.
(Arachidonic acid comes from omega−6 fatty acids, so humans on good diets should have less of this.)
Arachidonic acid becomes prostaglandin H2 inside the cell.
This is the step that aspirin blocks…
Aspirin inhibits cyclooxygenase, the enzyme responsible for this stage of prostaglandin synthesis.
Prostaglandin H2 is very unstable and spontaneously degrades within minutes – to either prostaglandin E2 or D2.
And, in yet another spontaneous step, though at a lower rate, prostaglandin D2 dehydrates into prostaglandin J2.
Prostaglandin J2 is the activating ligand for PPARγ, a transcription factor that creates mucin by replicating its DNA.
(PPARγ – Peroxisome proliferator-activated receptor gamma…the γ is the gamma.)
Activation of PPARγ sends the genetic code of the mucin out to the nucleus, encoded as mRNA.
And that gives it a template for mucin protein synthesis.
Invariably, PPARγ activation correlates with mucin production.
Besides taking aspirin to inhibit stone formation in that manner (by preventing mucin release), there are reliable ways to actively dissolve stones that have already formed!
You can use ursodeoxycholate, a bile salt that has been proven (in both in vivo and in vitro studies) to dissolve gallstones.
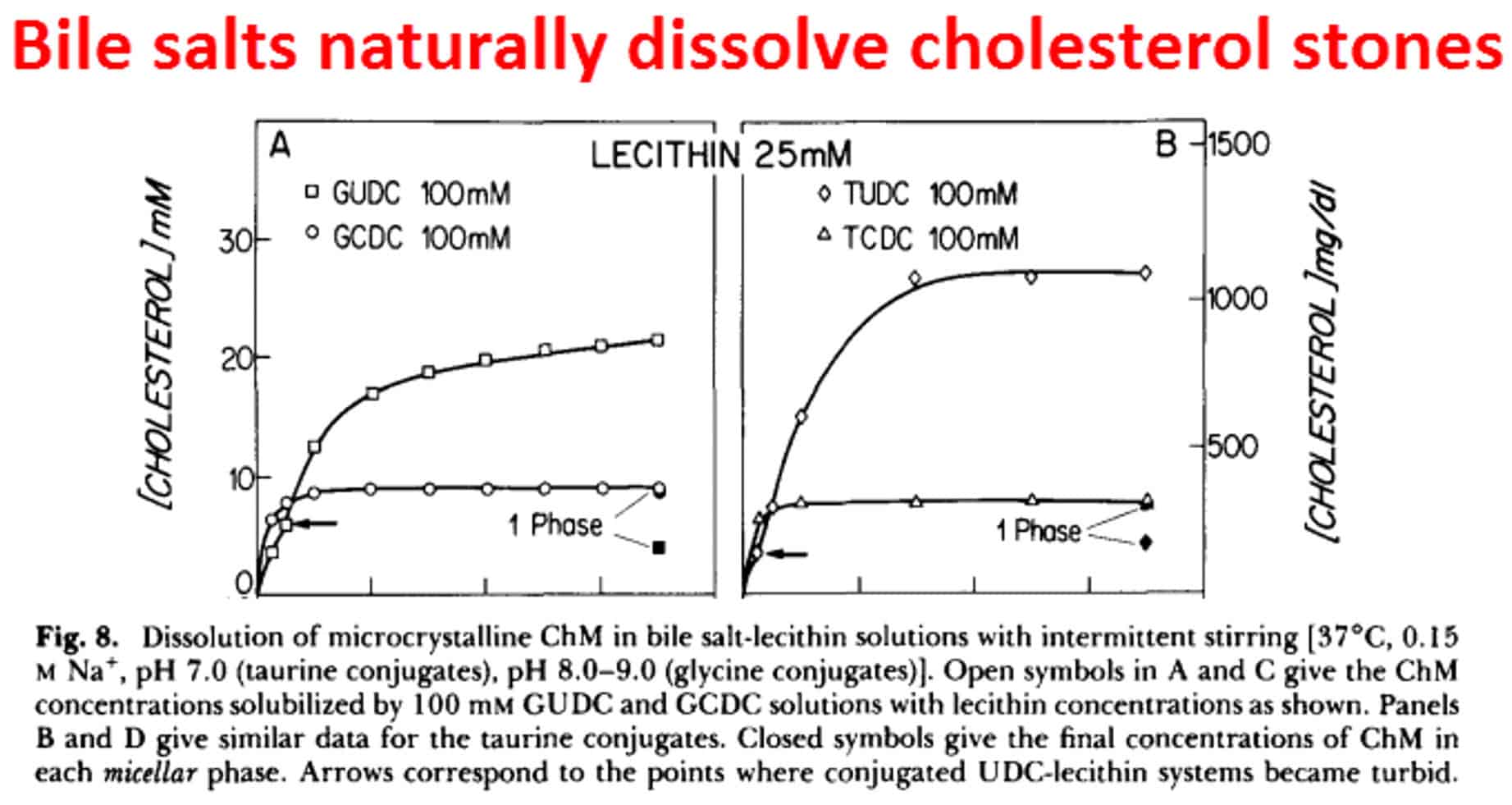
This method has been reliably demonstrated in people with gallstones, and has completely eliminated them in every case:
The researchers gave nine patients with gallstones 250-mg doses of ursodeoxycholic acid, twice a day – once after breakfast and then again after dinner.
They repeated ultrasound examination every 3 months – in all cases, the gallstones dissolved within 6 months.
All but the largest stone, 3.06 cm (1.2 inches) in diameter, which took between 6 and 9 months to dissolve.
“Gallstone 1 cm (.4 inch) or less in diameter disappeared within 6 months, and the largest stone 3.06 cm (1.2 inches) in diameter disappeared within 9 months.”
Now let’s bring taurine into this.
These researchers did not give the patients taurine with the ursodeoxycholic acid.
Taurine is necessary to conjugate ursodeoxycholate into the more efficient tauroursodeoxycholate.
In rats, simply taking taurine can completely prevent gallstone formation in all cases.
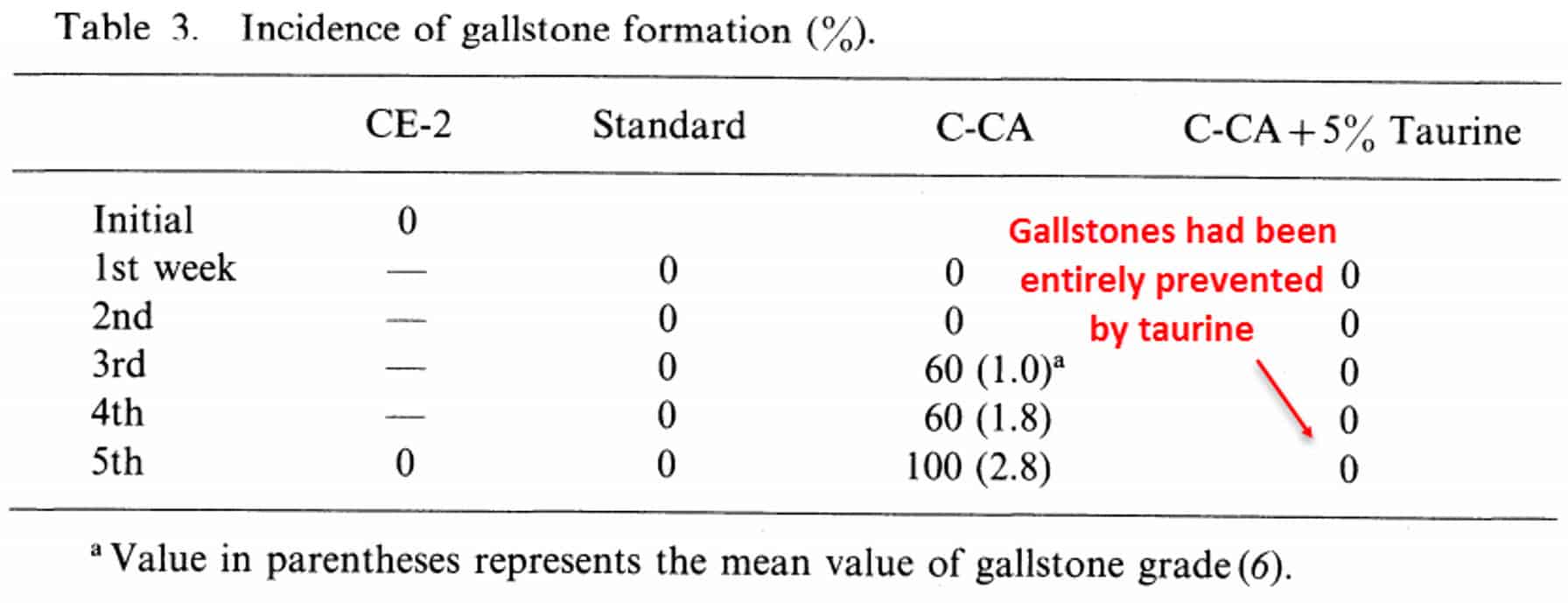
There’s no telling how fast gallstones can be dissolved using a ursodeoxycholine + taurine combination, but it should be substantially faster.
You can even buy preformed tauroursodeoxycholic acid online.
“Cholesterol is virtually insoluble in aqueous solution – but in bile, it is soluble by association with bile salts.”
The combination of aspirin, ursodeoxycholic acid, and taurine should be the most helpful to both dissolve gallstones and prevent them from occurring in the first place.
These three molecules are all capable of either preventing gallstone formation or dissolving stones already formed.
Who needs surgery? Besides the surgeons of course…
Taurine, ursodeoxycholic acid, and aspirin should all work in synergy – they are all completely safe, effective, reliable, and available at a reasonable price.
“Ursodeoxycholic acid is the principal bile acid in bears…normally constitutes only 1 to 2 percent of bile acid in humans. When ursodeoxycholic acid is given orally, it is absorbed, transported to the liver, and undergoes rapid and extensive biotransformation, predominantly involving conjugation with glycine and taurine.”
——Important Message——
Remember: Taurine is an amino acid that raises testosterone, heals your liver and helps with erectile problems
You can get a year’s supply of taurine for $15.
This is safe and effective and natural. You can also get it from shrimp and seafood. But you can get a lot more of it in the $15 bag that lasts a year.
Men who live to be 120 consume the most taurine in their diets… I even visited these men…
Here’s how these men use taurine to keep their powerful erections and their long-lasting health…

See how to use taurine to live longer and get more and better erections…
——————-

Leave a Reply